
You’re taking iron pills daily as directed, yet persistent fatigue, pale skin, and shortness of breath won’t fade. You’ve doubled your dose, switched brands, and even taken them on an empty stomach—yet blood tests still show low iron levels. When your body isn’t absorbing iron supplements properly, it creates a dangerous cycle of frustration and worsening symptoms. This isn’t just about swallowing a pill; it’s about complex biological processes that can fail for multiple reasons. If you’ve ever wondered why iron supplements aren’t working despite your best efforts, you’re facing a common but solvable problem that requires specific interventions beyond simply taking more pills.
Ignoring iron absorption issues has serious consequences. Unaddressed malabsorption can lead to severe anemia requiring blood transfusions, heart complications from chronic oxygen deprivation, and irreversible developmental delays in children. The good news? Most absorption problems stem from identifiable causes that respond well to targeted solutions. This guide cuts through the confusion to show you exactly how to diagnose why your body isn’t absorbing iron supplements, which evidence-based fixes actually work, and when to demand specialized medical intervention. You’ll learn the critical mistakes 90% of patients make when self-treating—and the precise steps to restore proper iron uptake within weeks.
How to Confirm Your Body Isn’t Absorbing Iron Supplements
Before assuming malabsorption, verify your iron status through proper testing. Many patients mistakenly believe their supplements aren’t working when they’re actually taking incorrect doses or timing them poorly. Request these specific blood tests from your doctor: serum ferritin (the most accurate iron storage indicator), transferrin saturation, and total iron-binding capacity. Crucially, avoid testing too soon after starting supplements—wait 4-6 weeks minimum for meaningful results. If ferritin remains below 30 ng/mL despite consistent supplementation, true malabsorption is likely occurring.
Why Standard Iron Tests Often Mislead Patients
Many doctors stop at hemoglobin checks, which only detect advanced anemia. By the time hemoglobin drops, iron stores are already critically depleted. A ferritin level of 15 ng/mL indicates severe deficiency even with normal hemoglobin. Additionally, inflammation from conditions like rheumatoid arthritis falsely elevates ferritin, masking true deficiency. If your doctor only orders hemoglobin tests when you report fatigue, insist on full iron studies including CRP to rule out inflammatory interference. Never rely on pharmacy finger-prick tests—they lack the precision needed for absorption diagnosis.
The Supplement Absorption Challenge Test
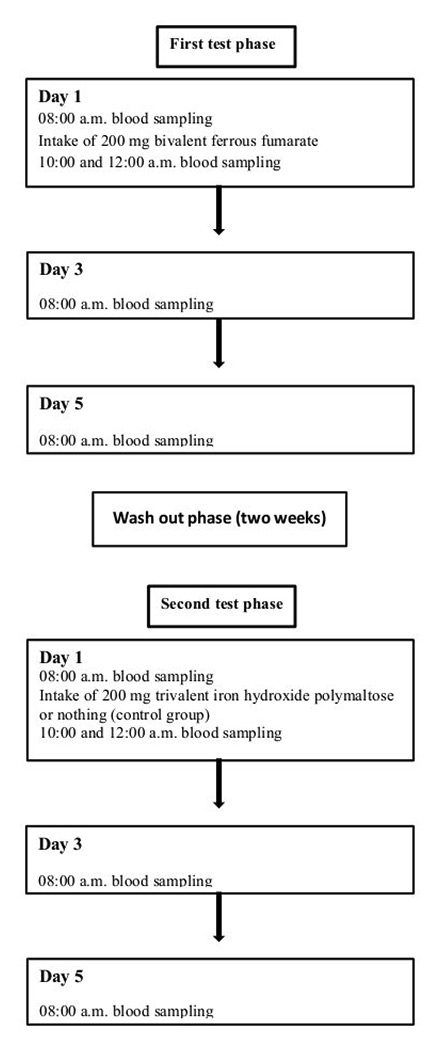
For definitive proof of malabsorption, request this clinical protocol: Take your regular iron dose with a timed blood draw before ingestion, then repeat tests at 2 and 4 hours post-dose. Healthy absorption shows a 50-100 mcg/dL serum iron spike within 2 hours. Flatline results confirm malabsorption—but this test requires coordination with your lab and is rarely ordered without patient advocacy. Bring this request to your appointment: “I’d like to schedule an iron absorption challenge test to evaluate my supplement efficacy.”
Fixing Common Iron Supplement Absorption Killers
Most patients waste months trying random solutions while ignoring these preventable absorption blockers. Each has specific countermeasures that restore uptake when properly implemented.
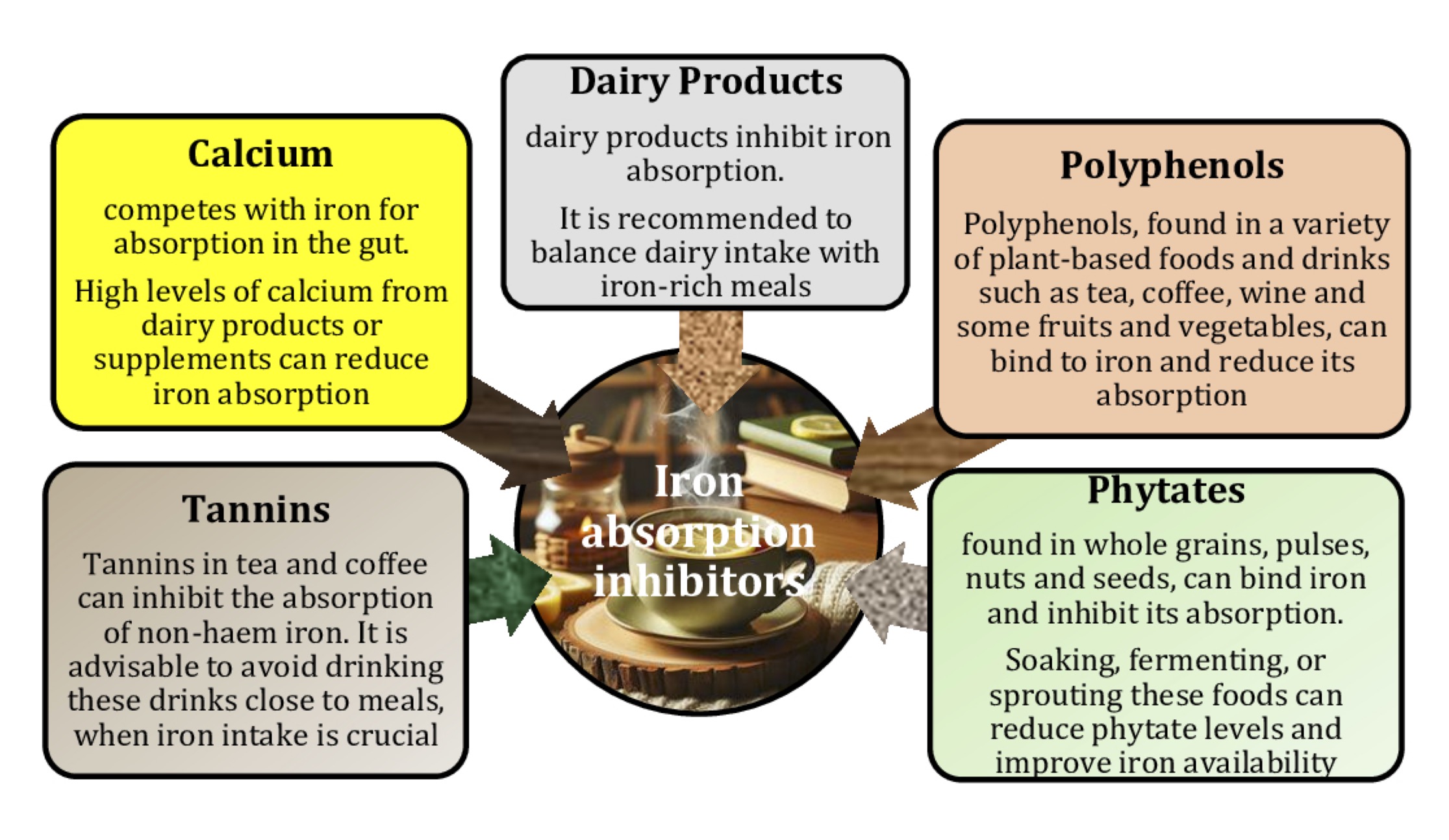
Neutralizing Dietary Iron Absorption Saboteurs
Calcium isn’t just in dairy—it hides in fortified plant milks, tofu, and even some bottled waters. Consume calcium supplements at least 4 hours away from iron doses, as 300mg calcium reduces iron absorption by 50-60%. Similarly, polyphenols in tea and coffee can slash absorption by 75% if consumed within 1 hour of supplements. The fix? Drink tea 2 hours after iron dosing, or add 60mg vitamin C (like half an orange) to counteract polyphenol effects. For phytate-rich whole grains, soak oats or bread overnight—this reduces phytates by 50% and boosts iron uptake.
Optimizing Supplement Timing for Maximum Absorption
Taking iron with food seems logical to avoid nausea, but it’s absorption suicide. Gastric acid is essential for converting iron to absorbable ferrous form, so take supplements 1 hour before meals on an empty stomach. If stomach upset occurs, try this pro move: Take iron with 100% orange juice (not from concentrate) for vitamin C’s protective effect against gastric irritation while boosting absorption 4x. For severe nausea, switch to ferrous bisglycinate—the only form proven effective with food according to clinical studies.
Medical Conditions That Block Iron Absorption (And Their Specific Fixes)
When standard fixes fail, underlying medical issues are likely sabotaging your iron uptake. These require targeted interventions beyond basic supplementation.
Solving Gut-Based Iron Malabsorption
Celiac disease damages duodenal villi where iron absorption occurs. If you have unexplained iron deficiency, get tested for celiac—even without digestive symptoms. The solution isn’t just gluten-free food—it requires strict avoidance of cross-contamination for 6-12 months to heal the gut. For H. pylori infections (present in 30% of iron-deficient adults), standard antibiotic therapy restores absorption within 3 months. Proton pump inhibitors like omeprazole reduce gastric acid by 90%, crippling iron conversion. Work with your doctor to switch to H2 blockers (like famotidine) which only reduce acid 60-70%, preserving enough acidity for iron uptake.
Hormonal and Systemic Absorption Barriers
Autoimmune conditions like rheumatoid arthritis trigger hepcidin production—a hormone that locks iron in storage. Standard iron supplements become useless when hepcidin levels are high. The fix requires treating the underlying inflammation with DMARDs before iron therapy succeeds. In heart failure patients, fluid overload dilutes iron markers—requiring IV iron that bypasses gut absorption entirely. For post-bariatric surgery patients, elemental iron supplements fail because duodenal bypass removes the primary absorption site. Switch to liquid iron polysaccharide complex absorbed in the jejunum.
When to Demand Advanced Iron Absorption Solutions
Oral supplements fail 30% of patients with true malabsorption. Don’t waste months in trial-and-error when these proven alternatives exist.
IV Iron Therapy: The Game-Changer for Stubborn Cases
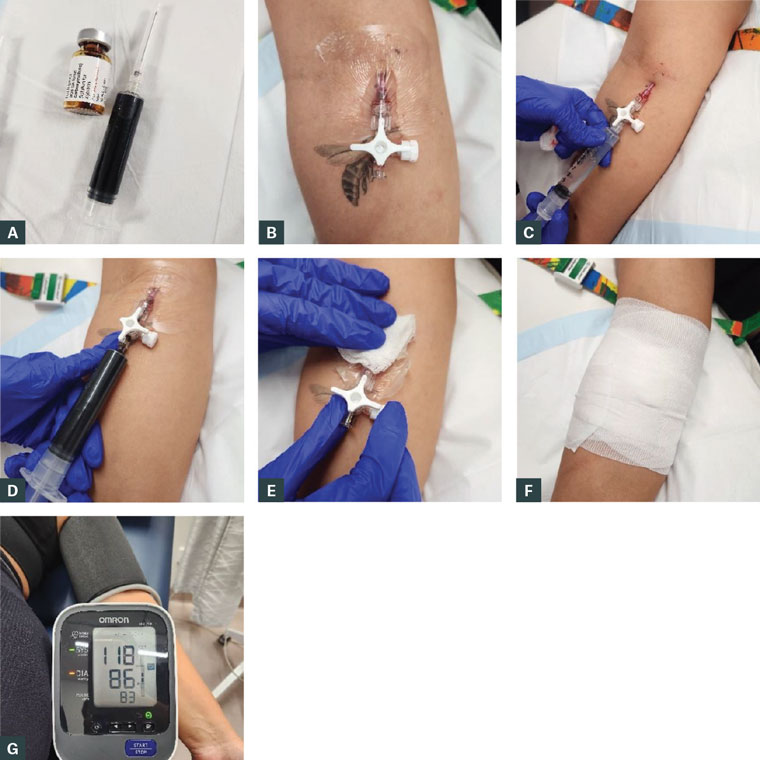
When ferritin stays below 20 ng/mL after 3 months of optimized oral therapy, IV iron becomes medically necessary. Modern formulations like ferric carboxymaltose deliver 1,000mg in 15 minutes with minimal side effects—no more multi-visit infusions. Benefits appear within 3-5 days as hemoglobin rises 1g/dL weekly. Best candidates: patients with active IBD, chronic kidney disease, or hepcidin-driven resistance. Insurance coverage requires documented failed oral therapy—track your supplement adherence and bloodwork meticulously to qualify.
The Ferrous Bisglycinate Advantage for Sensitive Systems
For patients who vomit with standard iron, ferrous bisglycinate (sold as Ferrochel®) is the gold standard. Its amino acid chelation allows absorption without gastric acid—critical for PPI users. Clinical studies show 90% better tolerance and 27% higher absorption than ferrous sulfate at equivalent doses. Take it with food to eliminate nausea while maintaining efficacy. Start with 25mg elemental iron twice daily—most patients need half the dose of traditional supplements.
Iron Absorption Maintenance Protocol
Prevent recurrence with this 4-part system used by hematologists:
- Post-recovery monitoring: Check ferritin every 3 months for 1 year—70% of patients relapse without maintenance dosing
- Strategic vitamin C pairing: 250mg with each iron dose (excess vitamin C degrades iron)
- Gut health foundation: Daily probiotic with Lactobacillus plantarum strain (proven to enhance iron uptake)
- Iron-friendly cooking: Use cast iron skillets for acidic foods like tomato sauce—adds 1-3mg elemental iron per serving
Critical warning: Never take iron supplements without confirmed deficiency. Unabsorbed iron feeds pathogenic gut bacteria and increases colon cancer risk by 20% in long-term users. Always retest ferritin 3 months after reaching target levels (30-50 ng/mL for most adults) to determine if maintenance dosing is needed.
Final Note: When your body isn’t absorbing iron supplements, the solution lies in methodical diagnosis—not random supplementation. Implement the supplement timing protocol and dietary adjustments immediately while pursuing medical testing for underlying causes. Track your symptoms and bloodwork in a dedicated journal to identify patterns. If standard approaches fail after 8 weeks, request a referral to a hematologist specializing in iron disorders—this isn’t stubbornness but necessary precision. Properly addressed, most absorption issues resolve within 3 months, restoring your energy and vitality. Remember: your iron journey requires partnership with knowledgeable providers, not persistence with ineffective pills. Start today by printing this guide for your next doctor’s appointment and demanding the specific tests outlined here.


