

Feeling constantly exhausted despite getting enough sleep? Struggling with brittle nails and pale skin that won’t improve? You might be one of the millions dealing with iron deficiency—the most common nutritional deficiency worldwide. Getting the normal iron supplement dosage right separates effective treatment from frustrating disappointment. Too little won’t rebuild your depleted stores, while too much brings uncomfortable side effects that make you abandon treatment. This guide reveals evidence-based dosing protocols, explains why standard recommendations are changing, and helps you navigate the complex journey from diagnosis to full recovery.
Iron deficiency develops silently over months or years before symptoms become noticeable. Your body needs iron to produce hemoglobin—the protein that carries oxygen to every cell in your body. Without adequate iron, your energy production plummets, cognitive function suffers, and your immune system weakens. While dietary iron forms the foundation of prevention, therapeutic supplementation becomes essential once deficiency sets in. Understanding the precise normal iron supplement dosage for your specific situation transforms confusing medical advice into a clear recovery roadmap you can follow with confidence.
Iron RDAs by Age: How Much You Really Need Daily
Your baseline iron requirements vary dramatically based on biological factors you can’t control. Knowing these standard requirements helps you recognize when dietary intake falls short and supplementation becomes necessary.
Infants and Children: Critical Growth Periods
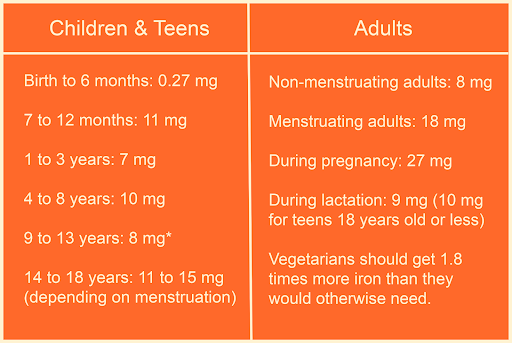
Breastfed infants need just 0.27 mg daily during their first six months—the perfect amount provided by breast milk alone. At seven months, requirements jump to 11 mg daily as solid foods are introduced. Toddlers (1-3 years) require 7 mg daily, while children aged 4-8 need 10 mg. Preteens (9-13 years) settle at 8 mg daily, setting the stage for the dramatic differences that emerge during adolescence.
Teenage boys and men over 19 need only 8 mg daily, while women between 14-50 require 18 mg due to monthly blood loss. Pregnancy dramatically increases needs to 27 mg daily to support fetal development and expanded blood volume. Lactating women need 9-10 mg daily, and after menopause, women’s requirements drop back to 8 mg—matching men’s requirements.
Vegetarian Iron Needs: The Bioavailability Gap
If you follow a plant-based diet, you need approximately 1.8 times more iron than meat-eaters. This difference stems from the bioavailability gap between heme iron (from animal sources) and nonheme iron (from plants). Heme iron absorbs more efficiently, while nonheme iron faces multiple absorption barriers.
Pro Tip: Boost your plant-based iron absorption by pairing spinach salads with citrus dressing or lentil soup with bell peppers. Vitamin C can increase nonheme iron absorption by up to sixfold, effectively closing the bioavailability gap when strategically combined.
Effective Oral Iron Therapy: Adult and Pediatric Dosing Guidelines
Oral iron remains the first-line treatment for most iron deficiency cases, but dosing protocols have evolved significantly based on new research about how your body actually absorbs supplemental iron.
Standard Adult Dosing: Why Less May Be More
Historically, doctors prescribed 100-200 mg of elemental iron daily in divided doses. However, recent research shows that 60 mg of elemental iron taken every other day often produces better results with fewer side effects. This surprising finding relates to hepcidin—the hormone that regulates iron absorption. After each dose, hepcidin rises and temporarily blocks further absorption. Spacing doses further apart actually increases total iron uptake over time.
Warning: Many over-the-counter supplements contain inadequate therapeutic doses. Multivitamins typically provide only 5 mg of iron—enough for maintenance but useless for treating deficiency. Always check the “elemental iron” content on the label, not just the total compound weight.
Pediatric Iron Dosing: Weight-Based Precision
Children require dosing based on body weight: 3-6 mg of elemental iron per kilogram daily. A 30 kg (66 lb) child needs 90-180 mg daily. Liquid formulations and chewable tablets make administration easier, but parents must use the provided measuring device—household spoons lead to dangerous dosing errors.
Iron Treatment Timeline: When to Expect Results and How Long to Continue
Restoring iron levels requires patience—you can’t reverse months of depletion in days. Understanding the realistic timeline prevents premature treatment discontinuation.
Hemoglobin Recovery vs. Complete Restoration
Hemoglobin levels typically begin rising within 2-3 weeks of consistent supplementation, with noticeable energy improvements within the first month. However, this represents only partial recovery. You must continue treatment for 3 months after hemoglobin normalizes to fully replenish ferritin stores—the body’s iron reserve. Stopping too early guarantees recurrence as depleted stores can’t sustain normal red blood cell production.
Monitoring Your Progress: Key Blood Tests
Your healthcare provider will track progress through periodic blood tests:
– Hemoglobin (typically checked every 4-6 weeks)
– Ferritin (measures stored iron)
– Transferrin saturation (indicates iron transport efficiency)
Normal ferritin levels should exceed 30 mcg/L, while values below 10 mcg/L confirm iron deficiency anemia. Inflammatory conditions can temporarily elevate ferritin, requiring additional testing for accurate assessment.
Stop Iron Supplement Nausea: Proven Strategies for Better Tolerance
Gastrointestinal side effects cause 10-20% of patients to discontinue iron therapy prematurely. These practical solutions maintain treatment adherence without sacrificing effectiveness.
Timing Is Everything: Maximizing Absorption
Take iron either first thing in the morning or between meals for optimal absorption. Avoid these absorption blockers for 2+ hours:
– Tea and coffee (reduces absorption by up to 60%)
– Calcium supplements and dairy products
– Antacids and proton pump inhibitors
– Whole grains containing phytates
Taking iron with a small amount of food reduces nausea while preserving sufficient absorption. Start with a lower dose and gradually increase over 1-2 weeks to build tolerance.
Liquid Iron Solutions: Preventing Teeth Staining
Dilute liquid iron with water or juice and sip through a straw positioned toward the back of your mouth. Brush with baking soda 30 minutes after taking your dose to prevent brown discoloration—this cosmetic issue is temporary and easily managed.
Why Your Iron Supplements Aren’t Working: 5 Common Causes
Consistent supplementation that fails to improve symptoms indicates underlying issues requiring investigation.
Ongoing Blood Loss: The Hidden Culprit
No amount of supplementation can overcome continuous blood loss. Common sources include:
– Heavy menstrual bleeding (menorrhagia)
– Gastrointestinal bleeding from ulcers or polyps
– Undiagnosed colon cancer
– Parasitic infections
Women with iron deficiency should receive gynecologic evaluation, while adults over 50 with new-onset deficiency require gastrointestinal investigation.
Absorption Inhibitors You Might Be Overlooking
Medications including proton pump inhibitors, antacids, and certain antibiotics significantly reduce iron absorption. Inflammatory bowel disease, celiac disease, and H. pylori infection damage the intestinal lining where iron absorption occurs. If you have these conditions, you may need higher doses or intravenous iron.
IV Iron vs Oral Supplements: When You Need Intravenous Treatment
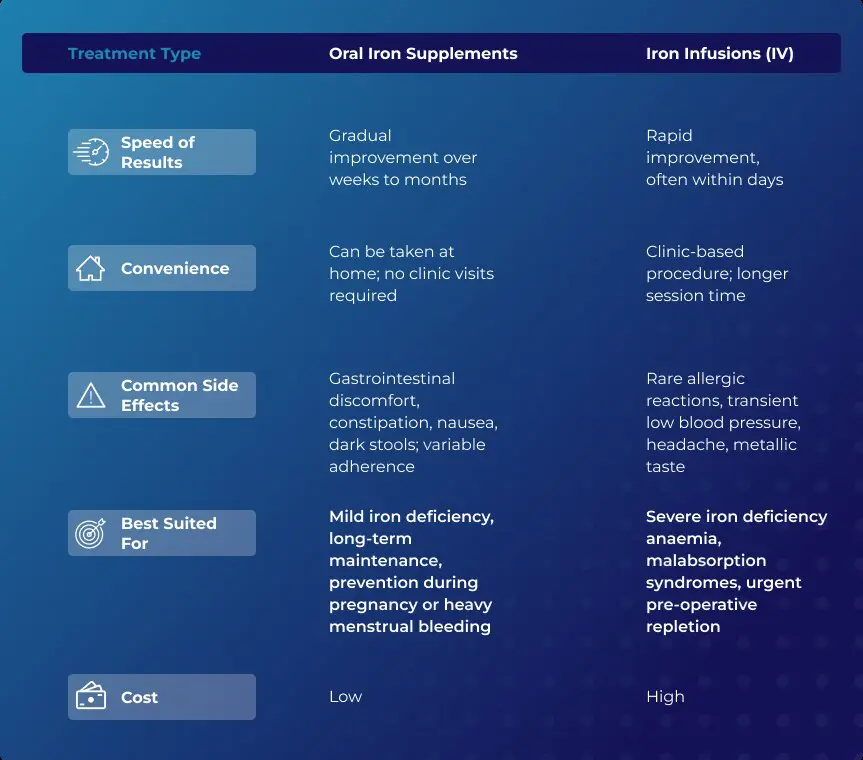
Oral iron fails for approximately 30% of patients due to intolerance or absorption issues. Intravenous iron provides a crucial alternative pathway.
Who Benefits Most from IV Iron
Consider intravenous treatment if you:
– Experience severe gastrointestinal side effects
– Have inflammatory bowel disease or celiac disease
– Require rapid iron restoration (hemoglobin <8 g/dL)
– Have ongoing blood loss exceeding oral replacement capacity
– Have congestive heart failure with iron deficiency
Modern IV formulations like ferric carboxymaltose allow larger single doses, reducing the number of required infusions. While IV iron carries a small risk of allergic reaction, serious complications are rare with current formulations.
Restoring healthy iron levels requires understanding your specific needs and following evidence-based normal iron supplement dosage protocols. The therapeutic range typically spans 60-200 mg of elemental iron daily, though many patients respond better to 60 mg every other day with fewer side effects. Children require weight-based dosing of 3-6 mg/kg daily. Crucially, treatment must continue for three months after hemoglobin normalizes to fully replenish depleted stores—stopping too early guarantees recurrence.
Remember that iron absorption depends heavily on timing—separate doses from coffee, tea, calcium, and dairy by at least two hours. If oral therapy fails despite proper adherence, investigate potential causes including ongoing blood loss, absorption disorders, or medication interactions. For those who cannot tolerate oral iron or require rapid restoration, intravenous treatment offers a safe, effective alternative. With the right normal iron supplement dosage strategy tailored to your specific situation, most patients experience significant improvement within weeks and complete recovery within months, returning to full energy and optimal health. Always consult your healthcare provider before starting or adjusting iron supplementation to ensure proper dosing based on your individual needs and laboratory results.


